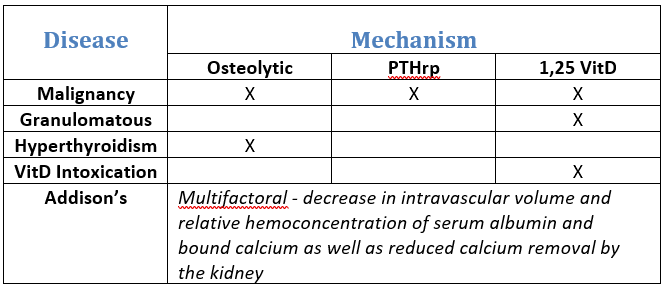
The term “hypercalcemia of malignancy” is routinely used when calcium is elevated and PTH is below normal, and for good reason— this situation is often a result of malignant neoplasia, particularly lymphoma, anal sac adenocarcinoma, or multiple myeloma. However, many other diseases can fall into this category such as granulomatous disease, hyperthyroidism, vitamin D intoxication, and Addison’s disease.
There are three major mechanisms by which hypercalcemia of malignancy can occur:
- osteolytic activity with local release of cytokines (including osteoclast activating factors)
- tumor secretion of parathyroid hormone-related protein (PTHrP)
- production of 1,25-dihydroxyvitamin D (calcitriol).
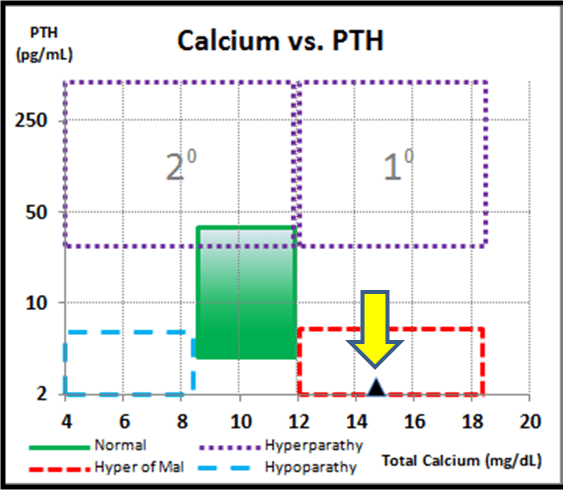
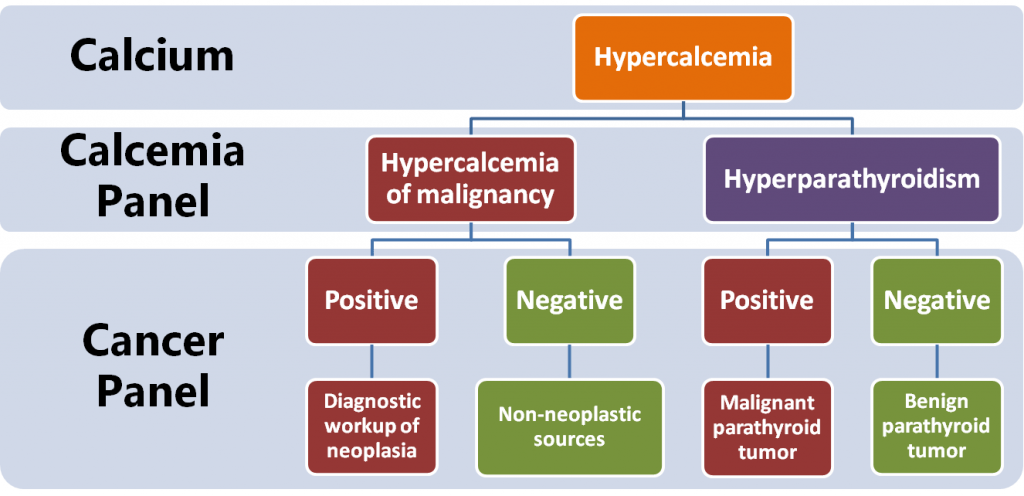
When a patient presents with hypercalcemia of unknown origin, a good place to begin is with a calcium and PTH measurement. If hypercalcemia of malignancy is present, the VDI Calcemia Panel report will plot within the lower red zone:
To rule in/out neoplasia as the reason for hypercalcemia, reflexing to the TK Cancer Panel will provide fast insight if neoplasia is suspect. If negative, other non-neoplastic causes can be further investigated.